TN 42 (01-24)
Exhibit 1 - SSA-545-BK (PLAN TO ACHIEVE SELF-SUPPORT)
This is a PDF of the SSA-545-BK for your use:
View In PDF
_____
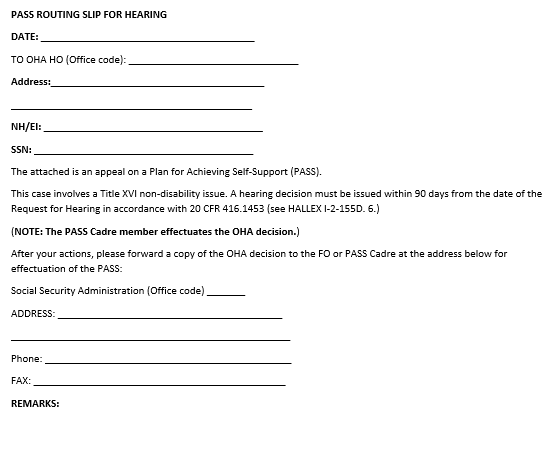
Exhibit 2 - PASS ROUTING SLIP FOR HEARING